কোভিড-নাইন্টিন রোগ – দ্বিতীয় ঢেউ-এর প্রস্তুতি
মোহাম্মদ আশরাফ হোসেন, ফেলো হিসেবে US FDA তে ৮ বছর কর্মরত ছিলেন, ফ্লোরিডা, ইউএসএ
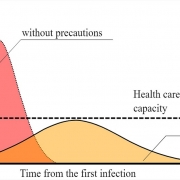
‘ঢেউ-এর পর ঢেউ’- ভাবতেই সাগরের ঢেউ বালুকাবেলায় আছড়ে পড়ার মনোমুগ্ধককর দৃশ্য মনে পড়ে। কিন্তু এপিডেমিওলোজী পরিভাষায় ঢেউ বা ওয়েভ-এর অর্থ সংক্রামক ব্যাধির প্রত্যাবর্তন, যা অনাকাঙ্খিত।
নীরব ঘাতক কোভিড-১৯ রোগ সংক্রমণ শুরু হয়েছিল গত বছরের ডিসেম্বরে চীনের ঊহানে; আর তা মাত্র কয়েক মাসে সারা বিশ্বে ছড়িয়ে পড়ে। এ রোগে এ যাবৎ আক্রান্ত হয়েছে ৩২ লক্ষাধিক মানবসন্তান, আর মাত্র কয়েক মাসে মৃত্যু হয়েছে প্রায় ২.৩ লক্ষাধিক। শিল্পোন্নত দেশ যুক্তরাষ্ট্রে মৃত্যু সংখ্যা সর্বাধিক, প্রায় ৬৩ সহস্র। মৃত্যুর মিছিলে শত-সহস্র যোগ হচ্ছে প্রতিদিন। যেমন, বিগত ২৪ ঘন্টায় যুক্তরাষ্ট্রে প্রায় ২ সহস্র (শুধু নিউ ইয়র্কে ৩০৬), যুক্তরাজ্যে ৬৭৪, মেক্সিকোতে ১৬৩, ব্রাযিলে ৩৯০ আর বাংলাদেশে অন্ততঃ ৫ জনের মৃত্যু হয়েছে। ইওরোপের বিভিন্ন দেশে শত-সহস্র সংক্রমণ ও মৃত্যু লক্ষণীয়। এরই মধ্যে আশার বাণী কিংবা গুঞ্জন শোনা যাচ্ছে- করোনাভাইরাস নাকি দূর্বল হয়ে গেছে। তারই ভিত্তিতে লকডাউন উপেক্ষা করার প্রবণতা বাড়ছে। যুক্তরাষ্ট্রের লকডাউন শিথিল এলাকার গাড়ি চলাচল বেড়েছে আর সী-বীচ, বোট ক্লাব আর পার্কগুলিতে বিপুল জনসমাগম হচ্ছে। লকডাউন প্রত্যাহারের দাবীতে জনসমাবেশ হয়েছে কয়েকটি শহরে। নতুন সংক্রমণ কিংবা মৃত্যুহারে সামান্য নিম্নগতি কিছুটা আশার সঞ্চার করলেও এ মুহূর্তে কোভিড-১৯ রোগ পরাস্ত কিংবা নিষ্ক্রমণের দাবী আর যাই হোক যুক্তিসঙ্গত নয়।
স্বাধীনতাহীন, গৃহবন্দী, অলস ও বেকার জীবন কেউ চায় না। কিন্তু ঊহানে কোভিড-১৯ এর প্রাদূর্ভাব শুরু হলে বাধ্যতামূলক লকডাউন, পিপিই বা সুরক্ষা সামগ্রী ব্যবহার ও সামাজিক দূরত্ব রক্ষার মাধ্যমে আড়াই মাস পর শহরবাসী মহামারীর কালো থাবা থেকে রক্ষা পেয়েছিল। এখন তারা সুস্থ-স্বাভাবিক জীবনযাপন করছে এমন দাবী করলেও বাস্তবে তা ঘটেনি; প্রায় অর্ধেক ব্যবসা প্রতিষ্ঠান এখনও বন্ধ। ফলে অর্থনৈতিক মন্দা দৃশ্যমান। এছাড়া নতুন করে সহস্রাধিক রোগ সংক্রমন ছাড়াও গত সপ্তাহে সেখানে ১৯ জন উপসর্গহীন রোগী পাওয়া গেছে।
লকডাউন ও সামাজিক দূরত্ব রক্ষা করতে গিয়ে যুক্তরাষ্ট্রে গত ৬ সপ্তাহে বেকারত্ব তিন কোটি ছাড়িয়েছে। সারা বিশ্বের বহু দেশে এখনো লকডাউন মেনে চলতে বলা হলেও গৃহবন্দী-দশা ও অর্থনৈতিক বিপর্যয়ের কারণে যুক্তরাষ্ট্রসহ বিভিন্ন দেশে যে ব্যাপক তোড়জোড় শুরু হয়েছে তা মঙ্গলজনক কিনা বলা মুশকিল। ভয়কে জয় করতে সাহসের প্রয়োজন, কিন্তু শত্রুকে দূর্বল ভেবে দূ;সাহসীর পরাজয়ের ঘটনা ইতিহাসে বিরল নয়। সুইডেন ও নরওয়ে প্রতিবেশী দেশ হলেও নরওয়ের তুলনায় সুইডেনে (লকডাউনে গুরুত্ব না দেওয়ায় ) সংক্রমণ ও মৃত্যুহার বেশী।
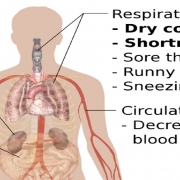
মনে রাখা দরকার, করোনাভাইরাস একটি আরএনএ-ভাইরাস যার সংক্রমণ ক্ষমতা ব্যতিক্রমী; এরা ভূখন্ড, ভাষা, জাতি, সতর্কবার্তা কিংবা ধর্মের বাছ-বিচার করে না। রোগ উপসর্গের অনুপস্থিতি কিংবা লক্ষণ রোগভিত্তিক না হওয়ায় পরীক্ষা-নিরীক্ষা ছাড়া শ্বাসতন্ত্রের এ রোগ নিরূপণ করাও কঠিন। আবার অত্যাধুনিক প্রযুক্তি ব্যবহার করে পিসিআর- টেস্ট কিংবা সেরোলজিক্যাল টেস্ট থেকে গুণগত (অর্থাৎ, পযিটিভ বা নেগেটিভ) ফলাফল পাওয়া গেলেও এদের কার্যকারিতা শতভাগ নিশ্চিত নয়। সেরোলজিক্যাল টেস্ট এর মাধ্যমে সাধারণতঃ করোনাভাইরাস অ্যান্টিবডি (প্রতিরোধী আমিষ) সনাক্ত করা হয়; টেস্ট পযিটিভ হলে সাধারণতঃ তা শুধুই সংক্রমণ ইঙ্গিত করে। অপরপক্ষে, করোনা ভাইরাস টেস্টের ফল নেগেটিভ হলে ব্যক্তি রোগমুক্ত কিংবা ঝূকিমুক্ত, এমন দাবী করাও অসঙ্গত। বরং উপসর্গহীন আক্রান্ত ব্যক্তি অথবা মিথ্যা-নেগেটিভ একজন বাহক মিথ্যা স্বস্তি নিয়ে অন্যদের সান্নিধ্যে এসে অজান্তেই কোভিড-১৯ রোগ বিস্তারে সহায়তা করতে পারেন। আবার, পর্যাপ্ত ইম্যুনিটি বা প্রতিরোধক্ষমতার অভাবে একবার সেরে উঠার পর কোন ব্যক্তি আবারও করোনাভাইরাসে আক্রান্ত হতে পারেন।
সার্বিক পরিস্থিতি নিয়ন্ত্রনে না এলেও এ সপ্তাহে যুক্তরাষ্ট্রের প্রায় দু-ডজন রাজ্যে লকডাউন শিথিল করে সতর্কভাবে পর্যায়ক্রমে ব্যবসা-কর্মস্থল খোলার প্রস্তুতি চলছে। তবে মধ্য-মে’র আগে নিউ ইয়র্কের অফিস-ব্যবসা খোলার সম্ভাবনা কম। ওয়াশিংটন ডিসির একজন প্রশাসক বলেছেন তিনি স্বল্প পরিসরে লকডাউন শিথিল করতে আগ্রহী। তিনি মনে করেন, রাজধানী ডিসি স্বাভাবিক হতে তিন মাস পর্যন্ত লেগে যেতে পারে। যুক্তরাষ্ট্রের করোনা পরিস্থিতি অগ্রাহ্য করা হলে কোভিড-১৯ এর প্রভাব আগামী শরত এমনকি শীতকাল পর্যন্ত দীর্ঘায়িত হতে পারে, এমন আশংকাও আছে।
প্রসঙ্গতঃ উল্লেখ্য, সংকুচিত সময়সূচি মেনে নিউ ইয়র্কের পরিবহণ সংস্থা ‘এমটিএ’ সাবওয়ে ও বাস সার্ভিস চালু রেখেছে। কিন্ত হটস্পট নিউ ইয়র্কে কোভিড-১৯-এ উল্লেখযোগ্য সংখ্যক স্বাস্থ্যকর্মী ছাড়াও অন্ততঃ ৮০ জন এমটিএ-কর্মী মৃত্যুবরণ করেছেন। এপ্রিলের ৯ এবং ৩০ সন্ধ্যায় নিউ ইয়র্কের এম্পায়ার স্টেট বিল্ডিং-এ এই দুই প্রথম সারির যোদ্ধাদের সম্মানে নীল আলোকসজ্জা করা হয়েছে।
জনবহুল বাংলাদেশে অন্যান্য দেশের তুলনায় কম হলেও নতুন কোভিড-১৯ রোগী সনাক্তকরণ ও মৃত্যু অব্যাহত আছে। সম্প্রতি ময়মনসিংহ ও নারায়নগঞ্জে বহু স্বাস্থ্যকর্মী কোভিড-১৯ এ আক্রান্ত হয়েছেন। পেশাজীবীদের মধ্যে ডাক্তার, সাংবাদিক ও পুলিশ সদস্যের মৃত্যু ঘটেছে। এছাড়া চট্টগ্রামে দুইজন ব্যক্তি দ্বিতীয় বার সংক্রমিত হয়েছেন। এসব সংবাদ দূশ্চিন্তার উদ্রেক করে। সীমিত আকারে বলা হলেও সহসাই লকডাউন শিথিল করে বহু সংখ্যক গার্মেন্টস শিল্প-কারখানা ও পবিত্র রমযানের কারণে ইফতারি/খাবারের দোকান চালু হয়েছে। গার্মেন্টস কর্মীরা চাকুরি বাঁচাতে নিকট ও দুরের জেলা থেকে কর্মস্থলে এসেছেন, অথচ যানবাহন চলাচলে নিষেধাজ্ঞা থাকায় অস্বাস্থ্যকর অবস্থায় ভ্রমণ করেছেন। স্বাস্থ্যবিধি মেনে চলার কথা বলা হলেও এসব কর্মী এবং খাবার ক্রেতা-বিক্রেতারা ভিড় করতে বাধ্য হচ্ছেন। এমতাবস্থায় নতুন করে রোগ সংক্রমনের আশঙ্কা বাড়ছে।
যা-ই হোক, সরকারী-বেসরকারী সমন্বিত উদ্যোগে প্রশাসন ও জনসাধারণের সহযোগিতায় এ নিম্নমুখী অর্থনীতির এ পরিস্থিতি থেকে উত্তরণ সম্ভব। তবে সদিচ্ছা কথায় সীমাবদ্ধ রেখে বসে থাকলে চলবে না। অতএব, পরিস্থিতি যথাযথভাবে মুল্যায়ন করে কর্মপদ্ধতি স্থির করতে হবে। যেমনঃ
– বিশ্ব স্বাস্থ্য সংস্থার নির্দেশিত নীতিমালা অনুসরণ করতে হবে।
– কুয়ারেন্টিন, সামাজিক দুরত্ব রক্ষা, ভ্রমণ (গমণাগমন) কিংবা লকডাউন নির্দেশনা সঠিকভাবে মেনে চলতে হবে।
– পরিস্কার-পরিচ্ছন্নতা বব্জায় রেখে, পিপিই ব্যবহার করতে হবে। এতে ব্যবহারকারী ও অন্যেরাও কিছুটা সুরক্ষা পাবেন।
– কেউ আক্রান্ত হলে বা রোগীর সস্পর্শে এলে পৃথক করে ১৪ দিন পর্যন্ত পর্যবেক্ষণ করতে হবে।
– রোগনির্ণয় সুযোগ বাড়াতে হবে। টেস্ট-এর ফলাফল যাচাই করে চিকিৎসা ব্যবস্থা দিতে হবে।
– সঠিক তথ্য প্রচার ও প্রসারে উদ্যোগী হতে হবে।
বিশ্বব্যাপী নিম্নমুখী অর্থনীতিকে চাঙ্গা করতে স্বাভাবিক কর্ম-জীবনে ফিরে আসার বিকল্ল নেই, কিন্তু আগুন নিভে গেছে ভেবে অগ্নিযোদ্ধারা তড়িঘড়ি করে ফিরে গেলে ফল যেমন খারাপ হতে পারে, তেমনই সংক্রমণ ঝুঁকি উপেক্ষা করে বেপরোয়াভাবে স্বাভাবিক জীবনে ফিরে এলে নতুন করে কোভিড-১৯ এর বিস্তার অর্থাৎ দ্বিতীয় ঢেউ এর আগমন ঘটতে পারে।